Women in Tanzania tend to pregnant at a very young age, this is closely related to their early marriage, and the severe sexual violence issue against the adolescent girls, as 7 percent of the women are pregnant before 15 years old. This group of people is also most affected by HIV/ AIDS. Childbearing at a young age, especially for those with infectious disease, entails a higher health risk for both mother and the child.
For a safe pregnancy journey, expecting mothers are recommended to attend 4 prenatal care visits and diagnose any sign of complication before delivery. For women living in a remote area, they can stay in the maternity waiting village 2 weeks ahead and deliver at the hospital. And those mothers need to come back to the facility and receive a postnatal check-up within 2 days of delivery. These procedures can reduce 80% of maternal death associated with preventable causes. However, the attendance of these maternal services at each stage remains relatively low. Only 15% of women attend antenatal visits before the fourth month of pregnancy and only 36% of births were performed in a skilled healthcare facility. The low attendance of maternal service also reflects the struggles of the current maternity system in Tanzania and raises the question of what are the factors that draw to the low utilization of maternal service.
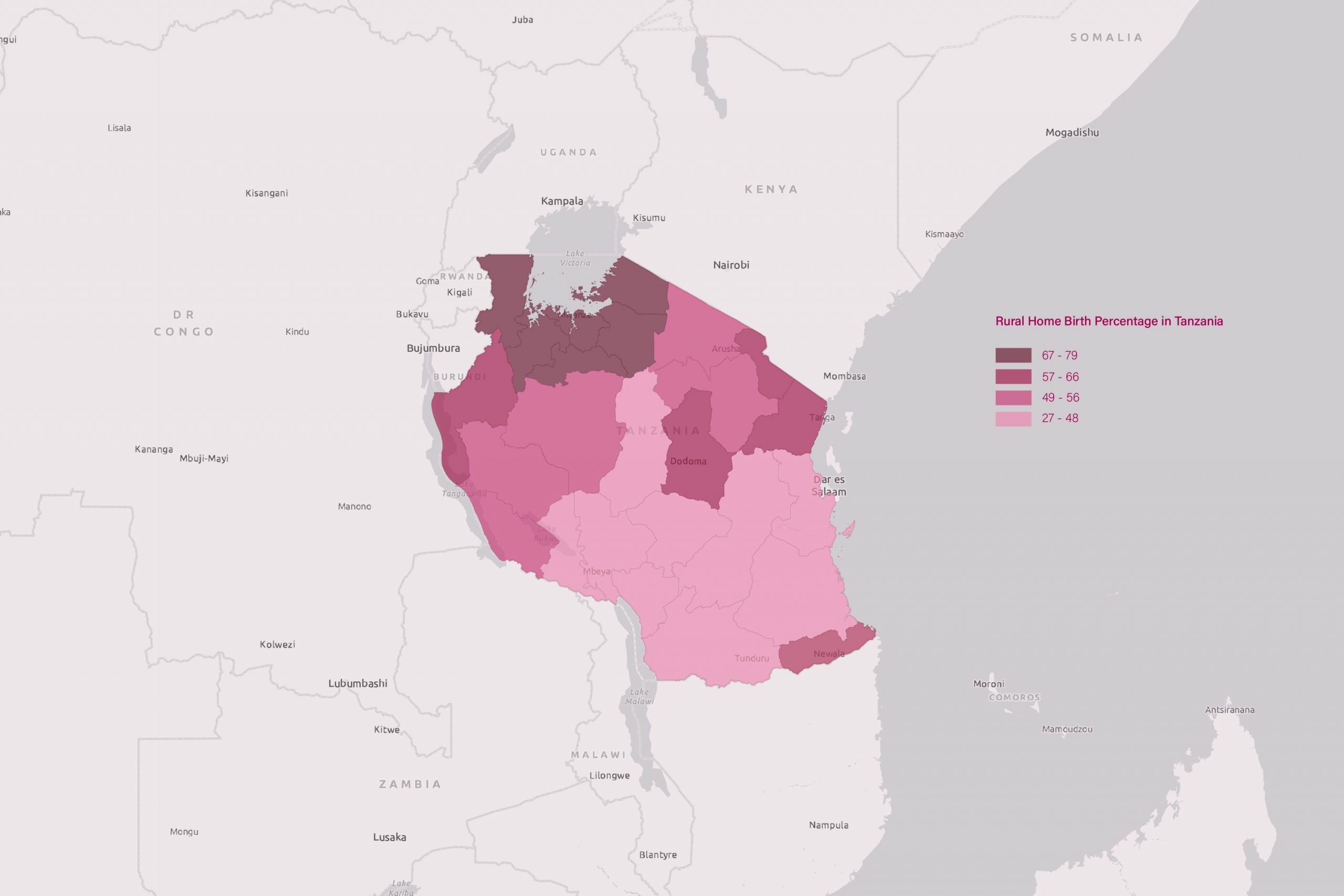
Infant and maternal mortality are highly related to the family living distance to the health facility in Tanzania. Although the travel time to the nearby health facility was largely within 1 hour as shown from the map, less than half of the health facilities are equipped with reproductive services. In some remote areas, travel times to a hospital exceed 12 hours from their home. Women often need to leave home several weeks ahead if they wish to deliver in a health facility. In addition, the current hospital bed ratio remains 0.7 beds per 1000 residents. Less than 5% of babies were delivered by cesarean section. This is partially due to a lack of skilled attendance and functioning blood banks at most facilities. Although some women recognize the importance of maternal care, the long travel distance and waiting time often keep those women away from seeking institutional care.

In a male dominated society, women are the primary caregivers at home and also need to carry their family’s agricultural needs. The acceptability of maternal care service is closely related to their culture and traditions. In the rural area, women need to be away from home for a few weeks if they choose to give birth in a health center. Being away from home means that they aren’t able to take care of their children and make the same amount of income as they would at home. In addition, some women simply dislike the concept of giving birth at a healthcare facility, because giving birth is a private family event and the current hospital could not provide adequate space for their family accommodation, hence lots of the women have to stay at the hospital by herself without any support.
The lack of accessible and available facilities, outdated accommodation for healthcare service, and low acceptability are the primary factors that lead to the low utilization of maternal service. Can architecture change the local’s perception on maternity service? Can a carefully designed maternity facility transform the traditional hospital birth experience?
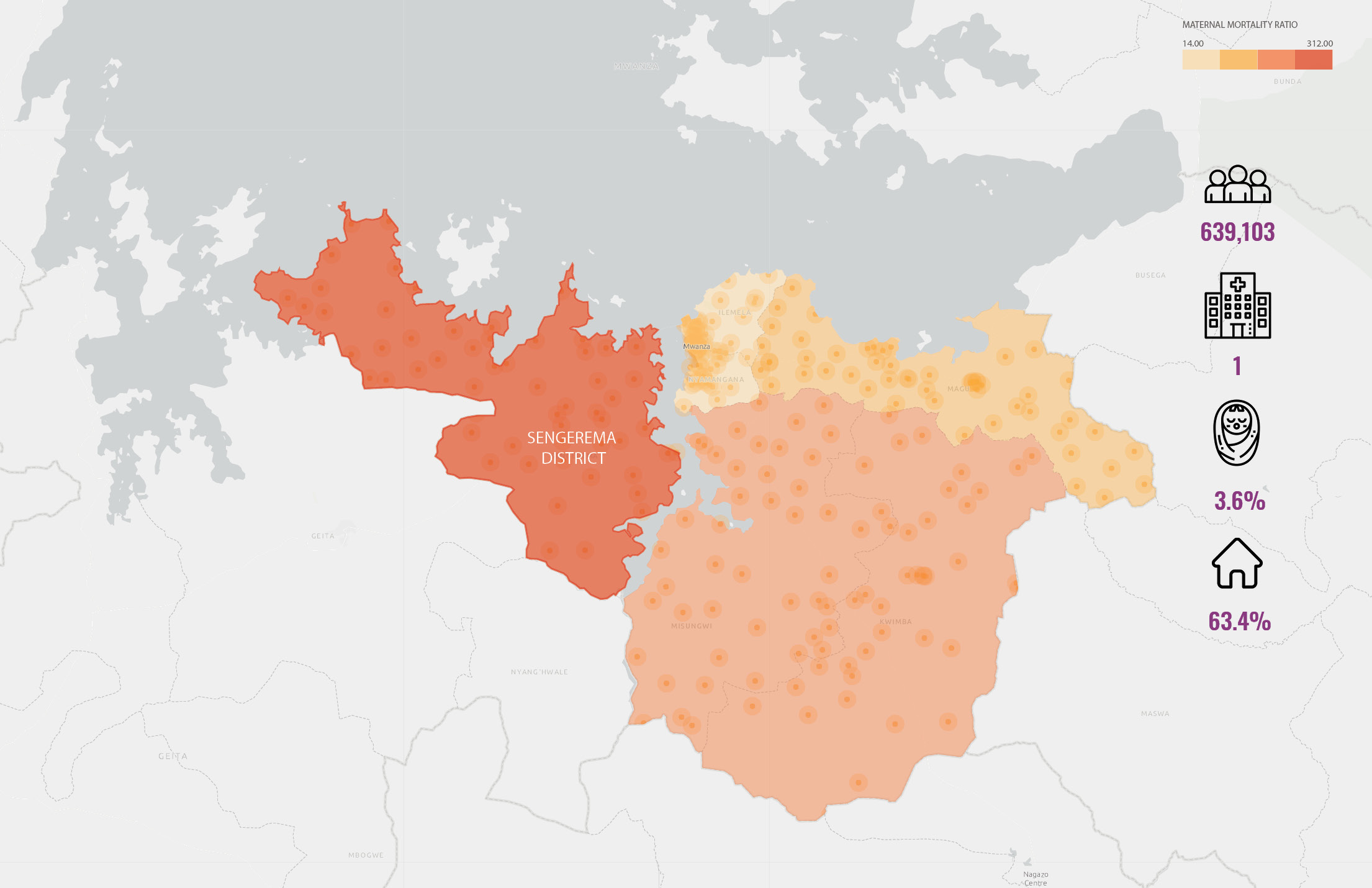
My thesis design and concept is to reassess the struggles of the current maternity system, and use three layers of strategies to improve the accessibility & availability, acceptability, and accommodation of the maternity facilities. The study area of this project will focus on the Sengerema district in the northern region of Tanzania. The population in the district is around 639 thousand, with only 1 hospital, 2 health centers available. The birth rate is around 3.6% with 63.4% of total birth performed at home.
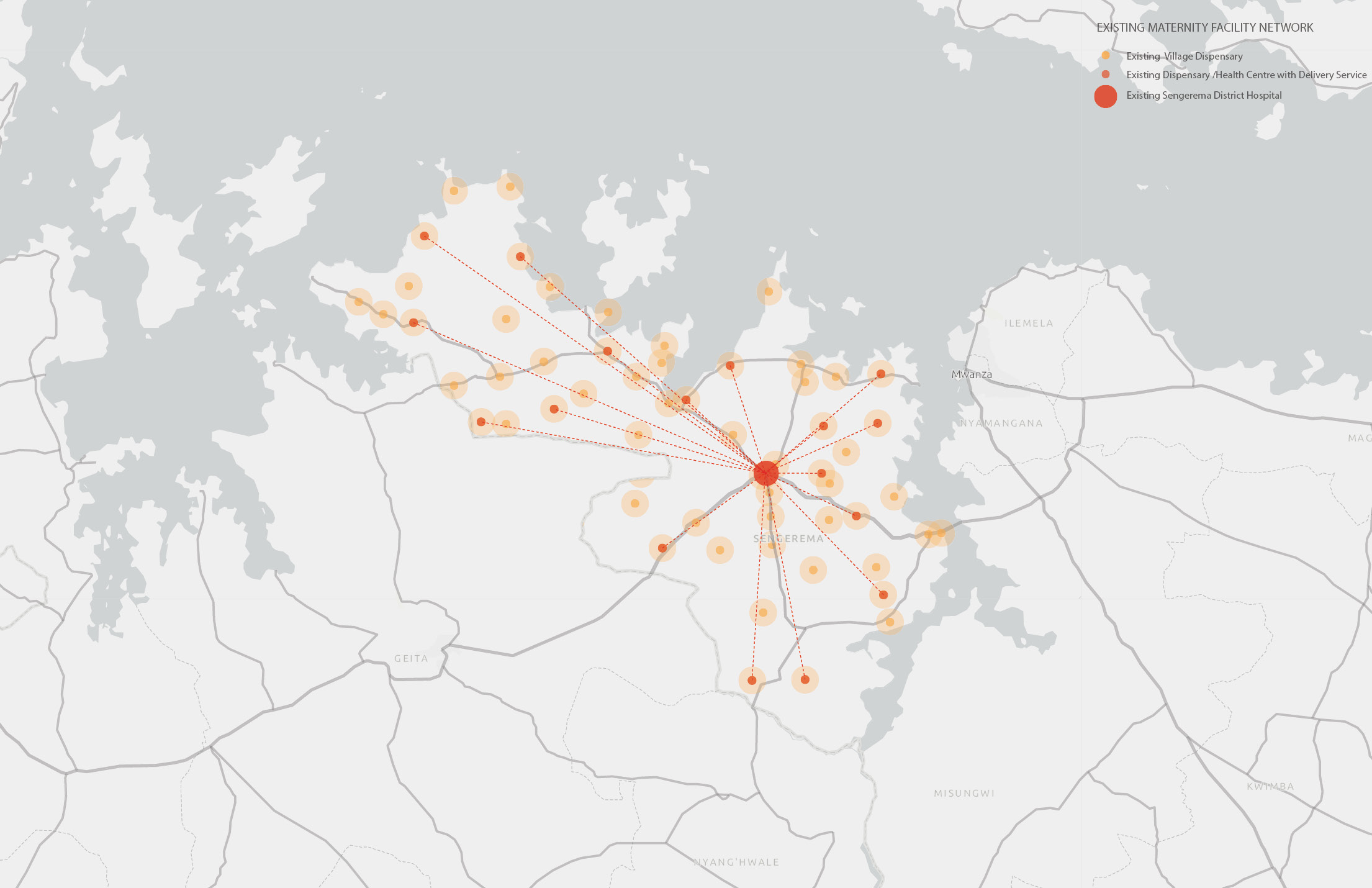
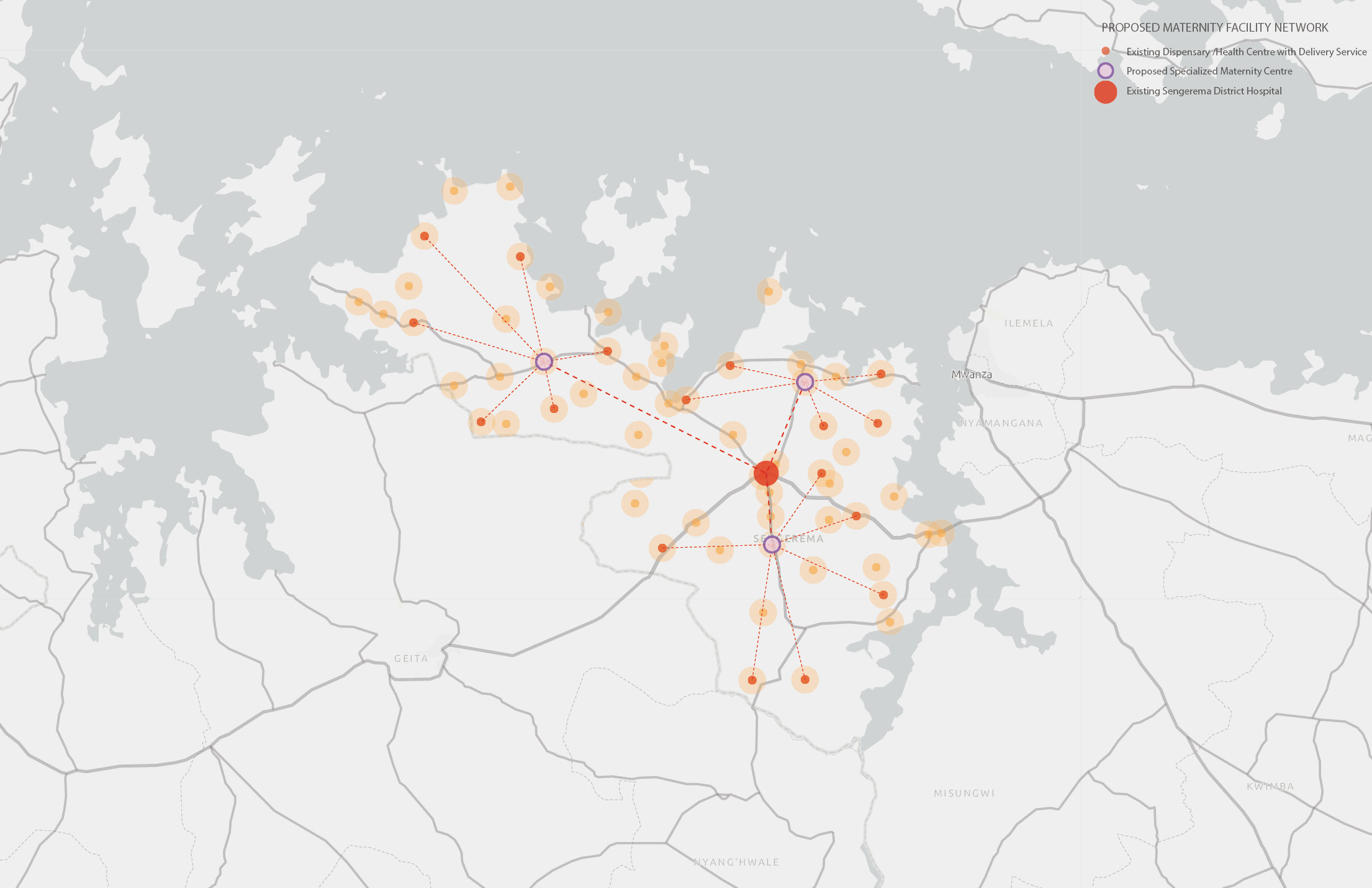
In the existing maternity network, all the local dispensaries would refer patients to the district hospital and result in an overload for hospitals. The first layer of strategy is to create a satellite network that could bring maternity facilities closer to the rural communities and shorten their travel time. But each of the satellite centers is still connected back to a district hospital as a mothership resource for emergency transfer and medical supplies.
Each of the satellite centers is also connecting to the existing dispensaries in the local communities and picking up patients from their referral point. A mobile clinic will be dispatched and visit all the surrounding villages in routine and perform antenatal exams and health care education to all the local residents.
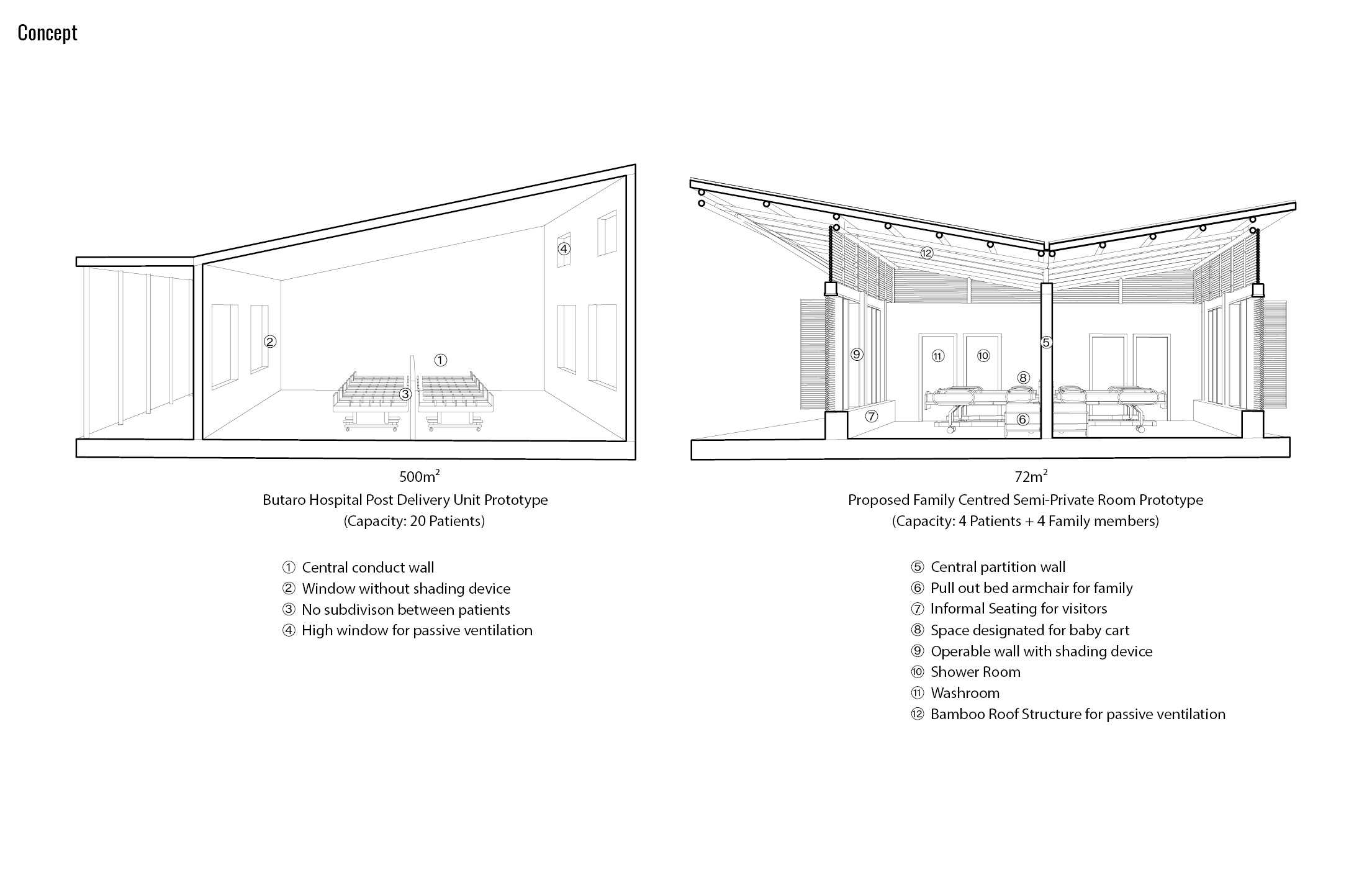
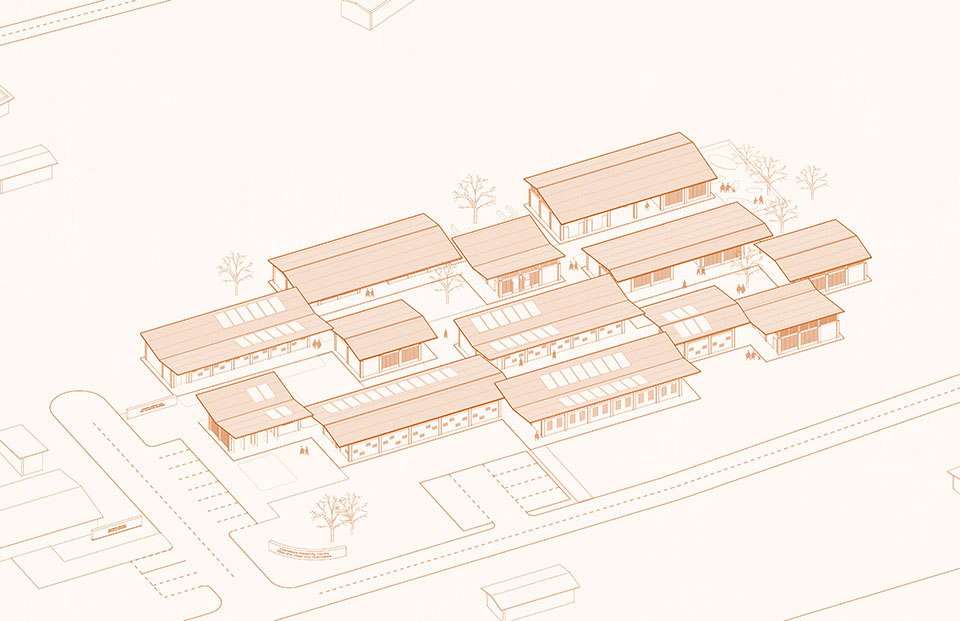
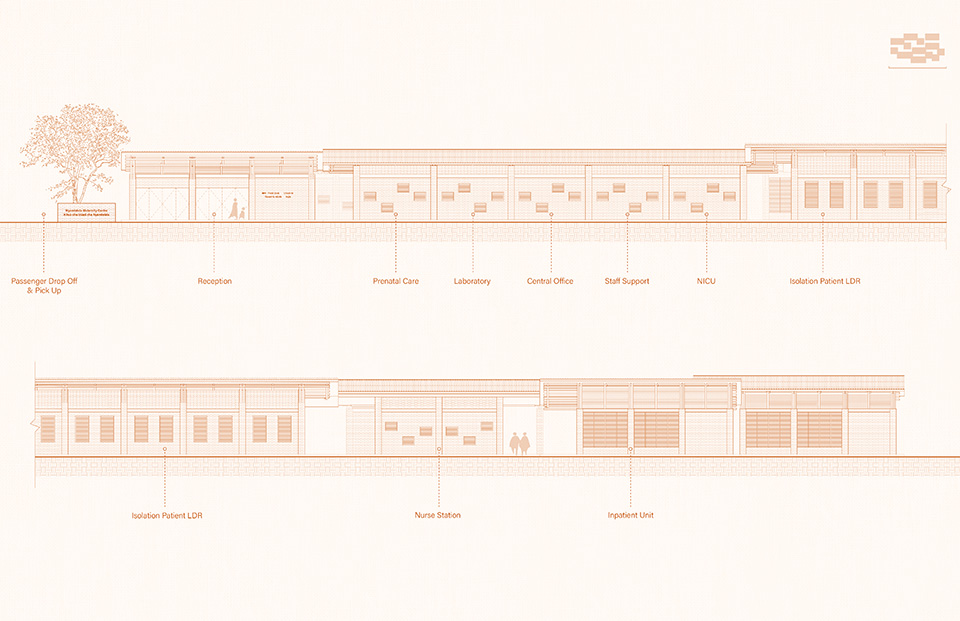
My second layer of strategy is to provide a de-institutionalized birth experience with family-centered care design which promotes and celebrates childbirth experience as a normal family process and encourages family members to stay with the expecting mother during their entire stay. Instead of having 20 patients laying in a big open room, I designed a semi-private room that can accommodate 2 patients and 1 family for each patient. And it is acuity adaptable to accommodate patients who come with their children. I added in a pull-out armchair for family accommodation and an informal seating area for family visits. With the operable window and shading device, all patients will have a view looking into the courtyard. Each room is equipped with one shower and one washroom. The bamboo structure will allow air exchange and passive ventilation even when the window is closed. The concept of family, support, and mental health is prioritized throughout the design process by creating a living space that is de-institutionalized, and closer to the residential scale.
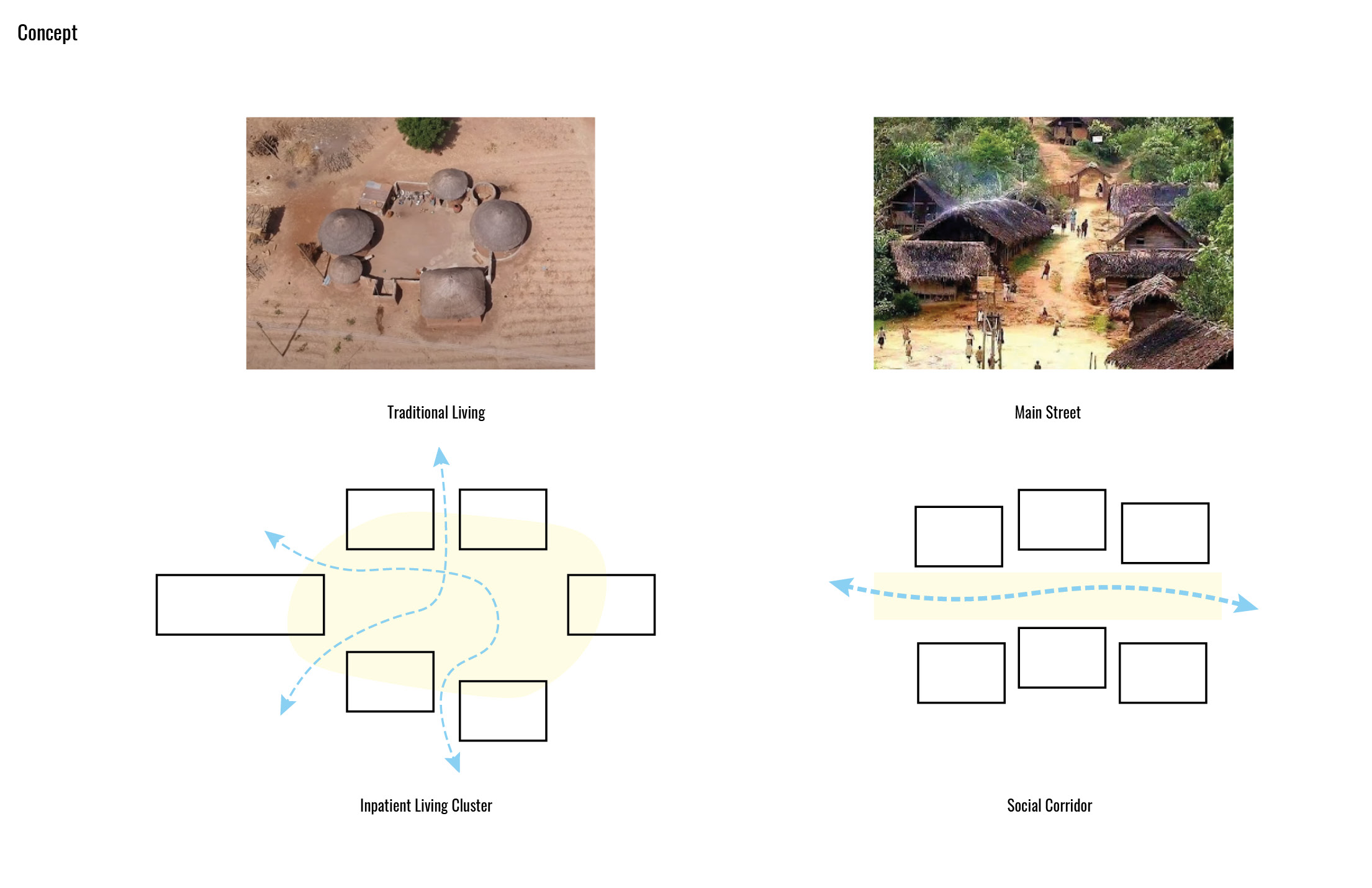
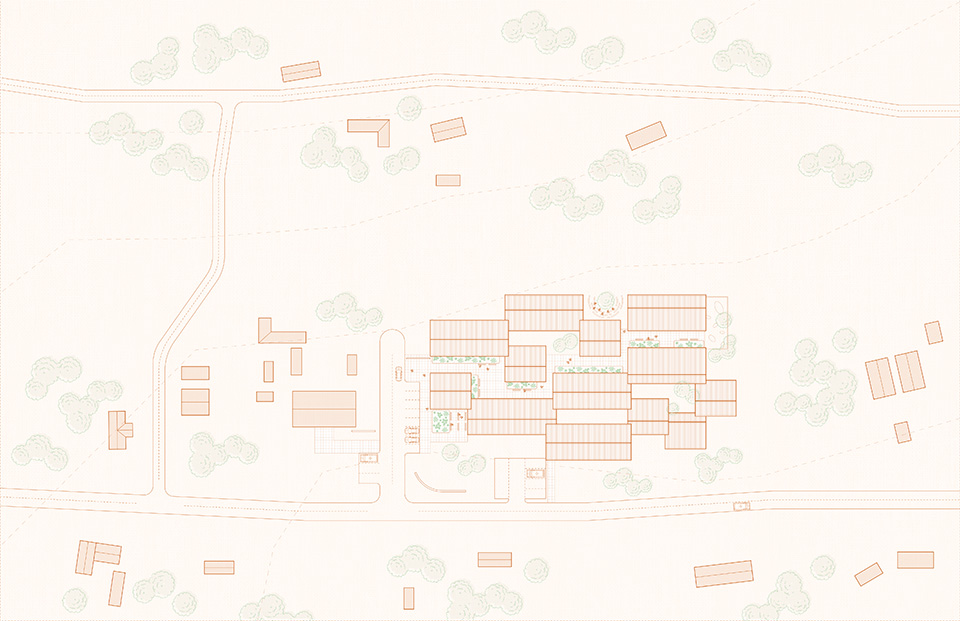
In the traditional ways of living in Tanzania, each household has an open courtyard that functions as their living room and social space. Each of the rooms such as the kitchen and bedroom is in different shapes and form a residential living cluster. By using the concept of traditional living, an inpatient living cluster typology is created in the proposed facility, where each of the inpatient units functions as a bedroom and surrounding an open courtyard. Each of the units is oriented asymmetrically so that it’s easier for wayfinding. And the concept of the main street within the village is being transformed into the social corridor within the facility, where different types of landscapes and social activities can happen.
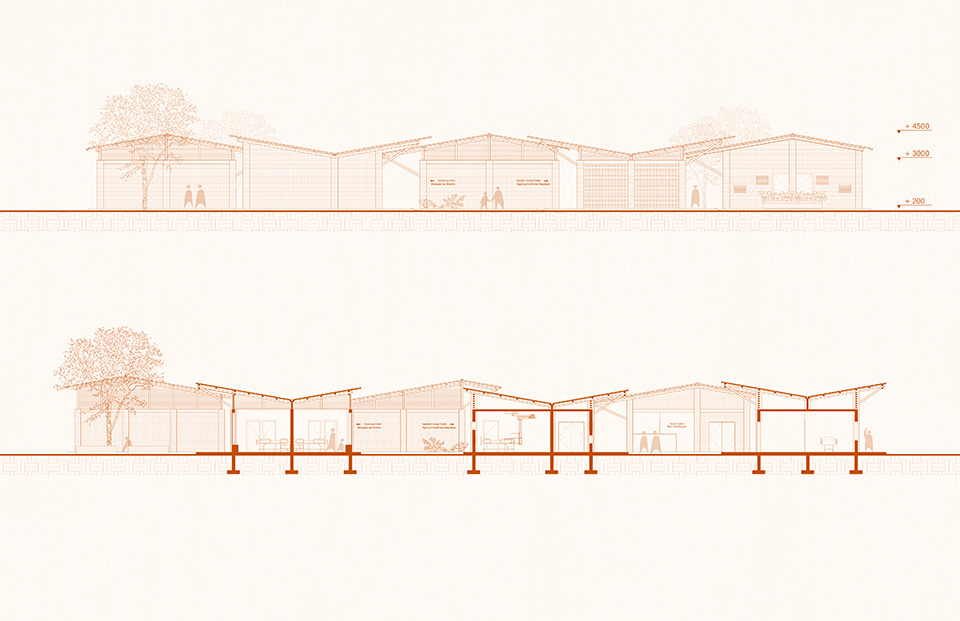
In this project I created two building types, one is for the service building which will require additional lighting and mechanics for medical equipment, so it will have an interior ceiling, and smaller operable windows painted with colors to reduce stress for patients during the delivery process. Another building type is the residential inpatient unit, which has larger operable windows so that patients can have a view to outside even when they lay in bed, and a bamboo roof structure with bamboo screen panel to allow air exchange for the room.
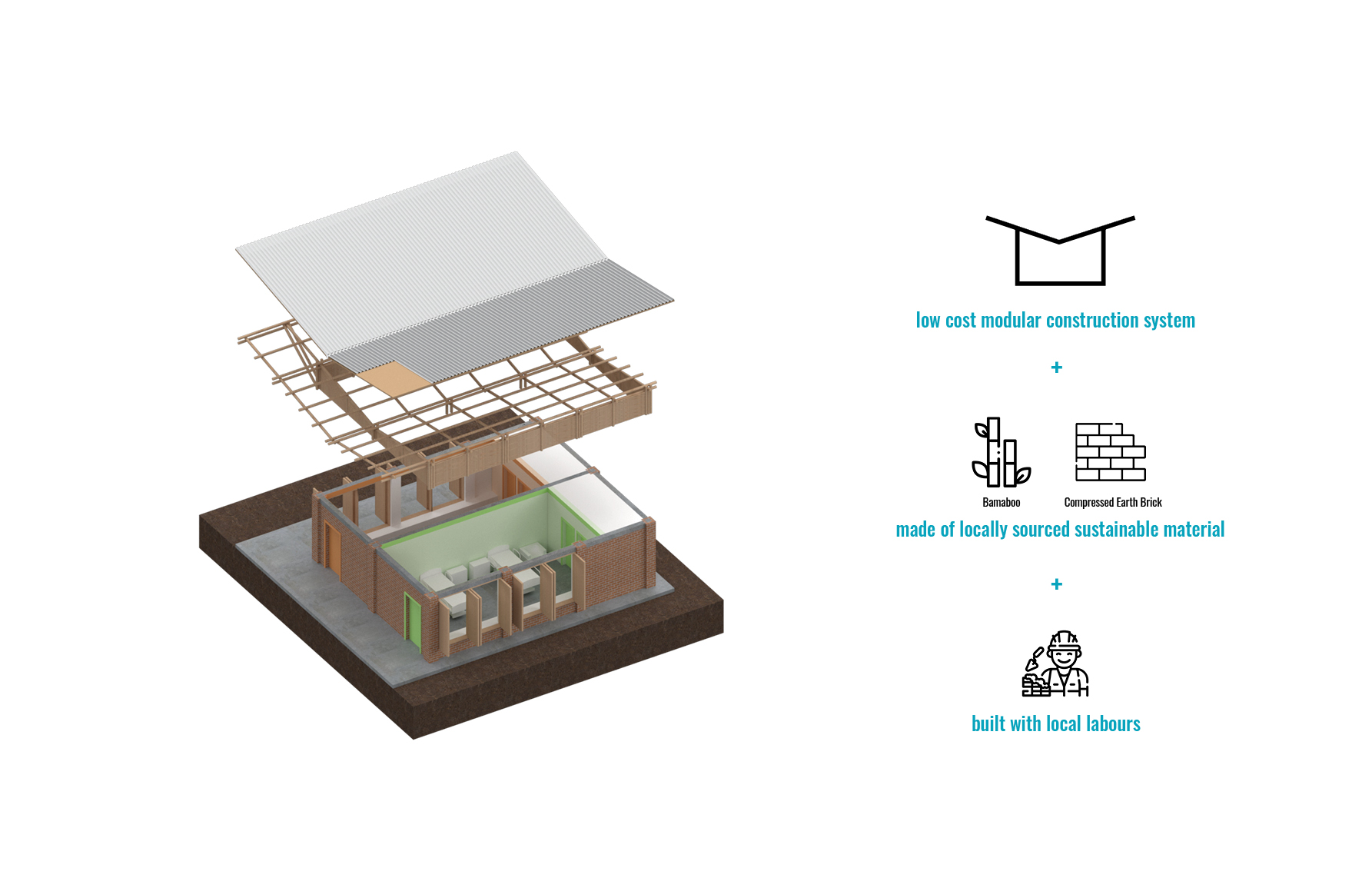
The building method will be in a modular system, with concrete moment frame and compressed mud brick, since Tanzania is currently experiencing a severe deforestation issue, the use of bamboo is promoted by the government is a more sustainable material, the roof is supported by the bamboo structure, and covered by woven bamboo sheet and metal corrugated sheet on top.